- The Morning Grind
- Posts
- 🦷 Cutters, restrictors, investors
🦷 Cutters, restrictors, investors
Good morning. A woman in Scotland was convicted of assault after attacking her dentist and trashing her office with a fire extinguisher. What great offense triggered this outburst, you ask? Apparently the patient did not take kindly to being informed that she was late and had missed her appointment. Almost makes you appreciate the patients who just no-show.
Inside this issue:
- Medicaid cuts start to bite dental budgets
- New study sheds light on smile simulation effectiveness
⏰ Your reading time today: 6 minutes 32 seconds
🏆 Enjoy your coffee break with Word of Mouth, a dental-themed word game inspired by Wordle.
MARKETS
📉 3D Systems Corp ($DDD) – 2.20 | -0.16 (6.77%)
📉 Align Technology ($ALGN) – 163.63 | -2.85 (1.71%)
📈 Colgate-Palmolive ($CL) – 91.89 | +6.89 (8.11%)
📉 Dentsply Sirona ($XRAY) – 12.21 | -0.44 (3.48%)
📉 Envista Holdings ($NVST) – 23.26 | -0.68 (2.84%)
📉 Henry Schein ($HSIC) – 75.31 | -2.02 (2.61%)
📉 Park Dental Partners ($PARK) – 17.26 | -2.06 (10.69%)
📉 Straumann Holding AG (STMN.SW) – CHF 93.36 | -2.56 (2.67%)
📉 Weave Communications ($WEAV) – 6.50 | -0.56 (7.93%)
Data is provided by Google Finance. Stock data reflects market close yesterday, showing changes over the past five days.
THE DRILL DOWN
📉 Affordable Care Act coverage falls by more than one million, according to new federal data, with experts warning that coverage is likely to drop further in coming months as enrollees realize their premiums have increased. "Affordable" has an asterisk this year.
🎤 Planet DDS announces the launch of AI Voice Perio, the first voice-powered periodontal charting system built within Denticon to help ensure consistent, reliable perio data across locations.
✂️ Half of Medi-Cal dentists might exit the California program, according to the California Dental Association (CDA), if proposed cuts to provider rates proceed, impacting the one-third of adults in the state that use Medi-Cal dental benefits.
🔍 The ADA pushes Congress for reforms in the dental insurance market, including standardized plan-level reporting, nonconsensual network expansion and rate leasing practices, and stronger claims administration standards.
🔍 EPA calls for public comments on its fluoride review, the next step in its assessment of the safety of adding fluoride to drinking water, something Department of Health and Human Services Secretary Robert F. Kennedy, Jr. has opposed. Nothing sparks public debate like a trace mineral.
🌎 Indiana’s House passes a bill to create a path for foreign-trained dentists to get a hygienist license, as long as they have a degree similar to a U.S. DDS or DMD, part of an effort to manage a shortage of hygienists.
☀️ New Mexico’s House of Representatives passes legislation to join the Dentist & Dental Hygienist Compact, clearing the way for the state to join 12 others in improving license portability for dentists and dental hygienists. Cleanings don’t stop at the state border.
Enjoying this newsletter? Subscribe for free (zero spam, just sharp dental insights) at www.themorninggrind.com
GOVERNMENT
2026 brings tough dental decisions for states

The "One Big Beautiful Bill Act" (OBBB) signed last July is now a reality hitting state budgets this month. Medicaid cuts and new work requirements are kicking in, forcing governors into high-stakes decisions that could spell trouble for dental practices.
Catch up: Through the OBBB, the federal government has tightened the purse strings on state budgets, ending enhanced funding for Medicaid expansion and capping the taxes states use to pump up reimbursement rates.
Shortfalls in funding for Medicaid are forcing states to either raise new revenue, reduce the scope of the program (either by restricting who is eligible or optional benefits), or lower reimbursement rates for providers.
Because adult dental benefits are optional under federal law, they are often the first target of cuts for states looking to find savings.
Beyond cuts to dental benefits specifically, the Congressional Budget Office estimates around five million adults will lose Medicaid coverage altogether under new eligibility rules.
Why it matters: There’s a good chance Medicaid changes that will impact your business are coming to a state you operate in this year. What those changes are will depend on geography, with states’ policy responses diverging into three camps:
The Cutters: California is the biggest state eyeing major cuts, with a proposal to eliminate dental coverage for undocumented adults and divert Proposition 56 funds (which supported rate increases) to plug budget holes. Idaho is planning to cut adult dental benefits, and Washington has already enacted rate reductions. North Carolina planned deep cuts but has since walked back that plan amid court challenges.
The Restrictors: Nebraska leads the charge on implementing the OBBB’s work requirements (eighty hours per month), aiming to have them in place by May 2026. Florida is tightening immigrant eligibility and piloting restricted programs. Expect these states to shed patients from their Medicaid rolls through bureaucratic hurdles and layers of eligibility restrictions.
The Investors: Surprisingly, some states are doubling down on certain aspects of Medicaid. Michigan is hoping to replace funding lost from federal cuts with a new tax in order to maintain Medicaid spending. Illinois is weighing bills to hike child dental rates by up to 50%. Pennsylvania is moving to restore root canal and perio coverage for adults.
Why it matters: Cuts and more stringent eligibility requirements are likely to show up in your clinic as patient churn and a margin squeeze.
With six-month redeterminations and work requirements, your Medicaid patient base is volatile. A patient approved in January might be dropped by July.
Cuts could make Medicaid participation financially unsustainable for many clinics. The California Dental Association warns 49% of dentists might drop the program if cuts proceed as planned in that state.
What you can do: If a meaningful segment of your patients are on Medicaid, don’t wait until cuts show up on your P&L. Here are a few things you can do right now to prepare:
Understand the playing field: Build a state exposure dashboard including visits, revenue, and margin, and tag each market’s risk level.
Automate eligibility: You cannot rely on monthly batch checks anymore. You need "day-of-service" verification. Invest in tools that check eligibility in real time before the patient sits in the chair.
Diversify your payer mix: If you are in a "Cutter" state, analyze your exposure and don't let Medicaid exceed a percentage of revenue you can afford to lose.
Explore other payment architectures: It may be worth looking into service agreements with Federally Qualified Health Centers—which aren’t exposed to Medicaid cuts in the same way—to protect volume.
Bottom line: If your organization serves patients on Medicaid, 2026 will be the year the effects of OBBB cuts and eligibility restrictions really start to bite. Preparing ASAP can soften the impact. If Medicaid is a pillar of your model, 2026 is your stress test.
Share this article: https://www.themorninggrind.com/p/2026-brings-tough-dental-decisions-for-states
BUSINESS BITES
👔 Notable leadership changes: The American Academy of Pediatric Dentistry announced Dr. Jessica Y. Lee as its next CEO, Dental Intelligence named Scott Johnson as its new CEO, and Alan Stein joins DentalXChange as Chief Solutions Officer.
🏢 Smile Partners USA opens its first de novo practice, signaling a strategic shift away from solely partnering with existing practices to fuel its growth. Maybe a rebrand to “Smile Builders” is in order?
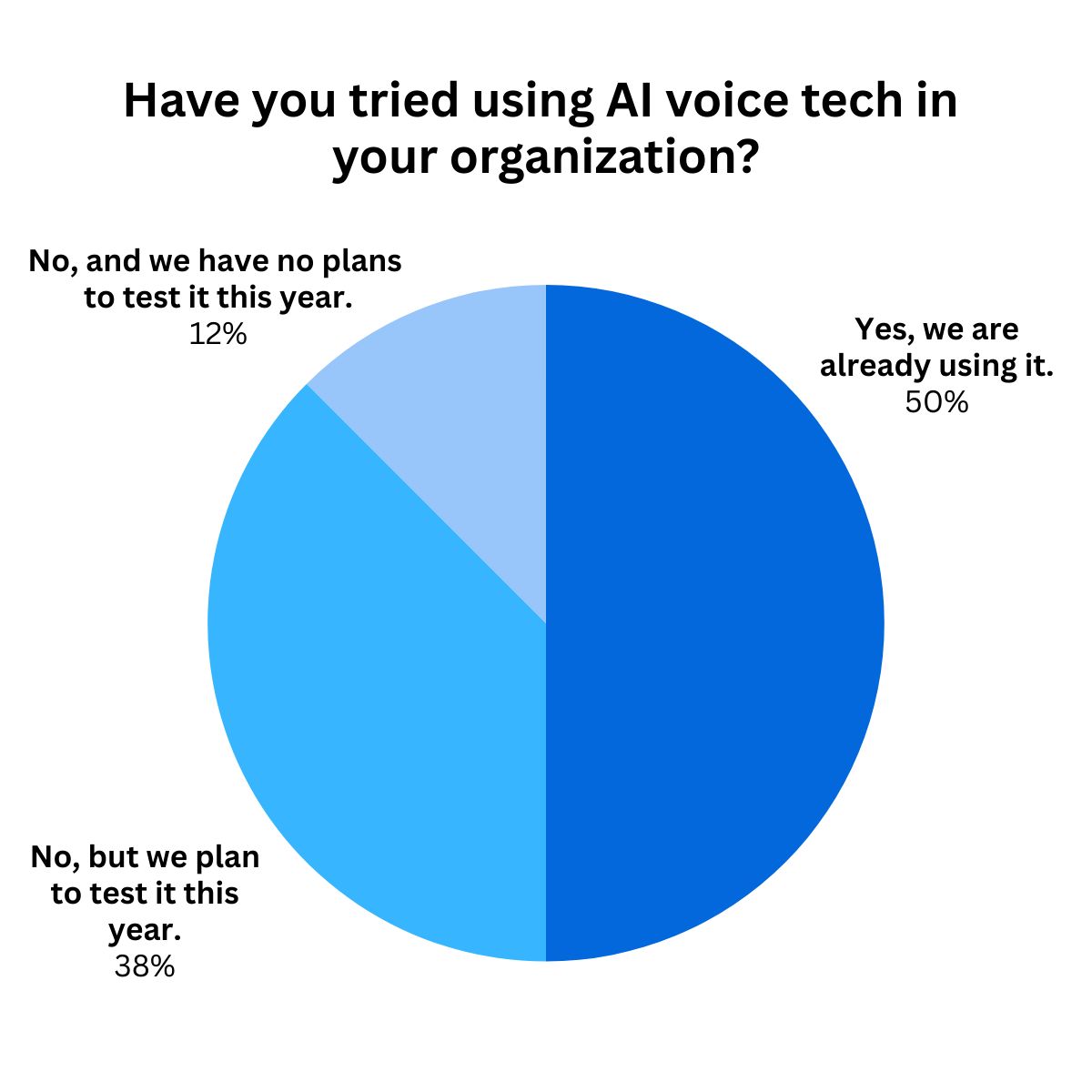
LAST ISSUE’S POLL RESULTS
TECH
New study finds smile simulations aren’t always a treatment acceptance home run

A decade ago, case presentation was a grayscale X-ray and a lot of trust. Now, with sophisticated visualization tech, it is a before-and-after preview of your patient’s own smile, right there in the chair.
But a new study reveals that without strong clinical guidance, a visualization alone isn’t usually enough to close a deal. Seeing is believing, but believing still takes a dentist.
Driving the news: A study published earlier this month evaluated the impact of the SmileView smile simulator on orthodontic treatment acceptance by patients. The simulation significantly improved how participants rated their potential smile, yet willingness to pursue orthodontic treatment actually slipped slightly (from 49% to 45%). The authors concluded that without clinical guidance, the tool didn’t move the needle on patient motivation.
Catch up: The findings come as AI visual simulations are moving from “cool demo” to chairside workflow, especially for ortho, cosmetic, and elective restorative procedures.
These simulations typically include outcome previews on a photo or scan, showing what someone’s smile will look like after a procedure.
Vendors are positioning these as acceptance engines. iTero, for example, markets Invisalign Outcome Simulator Pro as a chairside tool with in-face visualization and 3D model views “to help drive Invisalign treatment acceptance.”
Why it matters: The SmileView study is a warning label for rollout plans. Patients may love what they see in a simulation but still not go ahead with treatment if they don’t trust its credibility. If the preview looks unrealistic, looks only marginally better, or is not tied to a concrete treatment path, it can backfire.
Yes, but: Smile simulations address a real barrier, which is that patients struggle to value what they cannot visualize, whether it is alignment, esthetics, or future risk. A clear visual reduces cognitive load and makes the patient feel like they are deciding with you, not being sold to.
What you can do: If you’re going to use smile simulation tech, roll it out with the attention and care that you would any other clinical protocol.
Pilot one workflow, then expand. Start with ortho consults or elective esthetics. Baseline acceptance, time-to-schedule, and completion before deployment.
Standardize capture. Define photo angles, lighting, and who owns the step. “Random selfie” quality produces random results.
Don’t overpromise. Emphasize to patients that this is a visual aid to open a discussion about what’s realistic for their teeth. Then tie the visual to the treatment recommendation.
Bottom line: With one-third of dentists reporting that they aren’t busy enough, it’s no surprise that many clinics are looking for ways to drive up acceptance rates. Smile simulations can be an effective way to do that, but only when accompanied by real clinical guidance that makes patients confident that what they see in the sim is actually attainable.
🗳️ The Check-up:
⬆ VOTE: In your experience, do smile simulations improve treatment acceptance? |
CLINICAL NOTES
🦷 Scaling and root planing may effectively enhance tooth stability and reduce the risk of tooth loss in patients with gum disease, with a recent study showing the treatment demonstrated a significant reduction in tooth mobility at the 12-month follow-up.
📚 Patients with ADHD may have worse orthodontic treatment outcomes, a literature review found, with patients exhibiting reduced behavioral cooperation and increased risks of appliance breakage.
👶 Community water fluoridation was found to have no significant connection to changes in birth weight in new research from Columbia University, which analyzed data from over 11 million births.
🔍 Temporomandibular disorders (TMDs) are correlated with higher rates of addiction to nicotine, alcohol, and smartphones among university students, with the severity of TMDs also linked to greater levels of depression and anxiety. Jaw pain, scrolling, and stress—doesn’t sound like a great college experience.
FUN AND GAMES

BEYOND THE CUSP
Popular Mechanics rounds up the recent research on how oral health impacts longevity.
LeAnn Rimes is talking up a $10,000 plasma treatment to “clear micro-toxins” after her false teeth fell out on stage.
Scientists in China are prototyping a powder that can whiten teeth using just the vibrations of an electric toothbrush.
Any readers in Atlanta? Hawks forward Onyeka Okongwu needs some work done after taking a nasty elbow from Celtics star Jaylen Brown.
Just for fun: Try this viral Japanese cheesecake made with only two ingredients.